Summary
Shocking Study Reveals Mouth Cancer Costs Patients Over $2,000 Annually
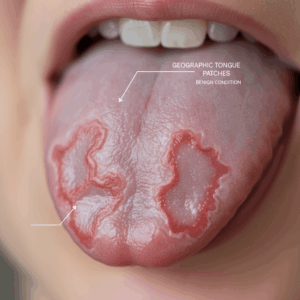
Oral cancer, commonly referred to as mouth cancer, affects various parts of the oral cavity including the lips, tongue, cheeks, and floor of the mouth. It predominantly presents as squamous cell carcinoma and is strongly linked to risk factors such as tobacco use, excessive alcohol consumption, poor oral hygiene, chronic irritation, and human papillomavirus (HPV) infection. The disease carries a high global burden, with incidence and mortality rates notably elevated in low- and middle-income countries such as Pakistan, Brazil, and India, and an increasing prevalence among younger populations in Africa, the Middle East, and Asia.
This comprehensive study highlights the substantial economic burden that oral cancer imposes on patients worldwide, revealing that individuals affected by mouth cancer often incur over $2,000 in out-of-pocket expenses annually. Treatment costs escalate dramatically with disease progression; advanced-stage cancers require more complex and costly interventions, resulting in treatment expenses up to 373% higher than early-stage care. Additionally, non-medical expenses—including travel, caregiving, and ancillary services like dental care and physiotherapy—significantly contribute to patients’ financial strain, frequently exceeding coverage provided by insurance and health systems.
The financial impact of oral cancer is further exacerbated by socioeconomic disparities and systemic factors such as insurance coverage gaps and healthcare infrastructure variability. These issues lead to inconsistent support for essential non-medical costs and contribute to catastrophic health expenditures, which can cause psychosocial distress and negatively affect treatment adherence and quality of life. Despite these challenges, the heterogeneity and methodological limitations of current cost-of-illness studies complicate efforts to develop standardized economic evaluations and cost-effective resource allocation strategies.
To address these concerns, the study underscores the critical importance of early detection, standardized cost reporting, and integrated care models that encompass financial counseling and support for non-medical expenses. By improving access to early-stage diagnosis and reducing out-of-pocket burdens, especially for vulnerable populations, healthcare systems can mitigate the overall economic and health impacts of oral cancer globally.
Background
Oral cancer, also known as mouth cancer, primarily affects the tissues of the lips, tongue, cheeks, floor of the mouth, palate, and sinuses, with squamous cell carcinoma being the most common malignant type. The disease is strongly associated with risk factors such as tobacco use, heavy alcohol consumption, poor oral hygiene, chronic irritation, and human papillomavirus (HPV) infection. Geographically, the highest incidence rates occur in low- and middle-income countries including Pakistan, Brazil, and India, and there is a noted increase in cases among younger populations, especially in Africa, the Middle East, and Asia.
Early detection of oral cancer is critical due to its significant impact on survival rates and treatment costs. The disease is often diagnosed at advanced stages, with stage IV representing the most severe form involving spread to distant organs or multiple lymph nodes. Early-stage (I and II) oral cancer patients have a five-year survival rate of approximately 80%, while advanced stages (III and IV) see survival rates drop to 50% or less, necessitating more aggressive and costly treatment approaches. Unfortunately, many patients are diagnosed late, which compromises survival and results in higher out-of-pocket treatment expenses.
Socioeconomic factors and disparities play a substantial role in the burden of oral cancer, affecting incidence, mortality, and disability-adjusted life years (DALYs) across different regions and populations. Patients from lower socioeconomic strata and those with inadequate dietary intake are at greater risk, underscoring the need for effective public health policies that promote early detection through education, opportunistic screening, and primary care integration.
Treatment costs for oral cancer vary significantly depending on the stage at diagnosis. Advanced stages require more complex interventions, such as surgery, radiotherapy, chemotherapy, and prolonged hospital stays, which substantially increase the economic burden on patients and healthcare systems. Studies show that advanced-stage treatment costs can be from 21.9% up to 373.3% higher than those for early stages, and recurrent tumors are also considerably more expensive to manage. These financial challenges impact patients’ quality of life and survival, highlighting the importance of early diagnosis and cost-effective care strategies in reducing the overall economic and health burden of oral cancer.
Study Details
This study presents a comprehensive and critical overview of the cost-of-illness (COI) analyses related to oral cancer worldwide, emphasizing the substantial financial burden it places on societal and public health expenditures. The investigation employed the PEO (Population, Exposure, Outcome) framework to guide the search strategy, considering any individuals or groups exposed to oral cancer, including lip cancer (LC), oral cavity cancer (OCC), and oropharyngeal cancer (OPC), without restrictions on age, sex, race, or socioeconomic status.
Data on the global burden of oral cancer were analyzed from 1990 to 2021, covering annual incidence, mortality, and disability-adjusted life years (DALYs) across 204 countries. These metrics were assessed using age-standardized rates alongside the Socio-demographic Index (SDI) to evaluate the influence of development factors on oral cancer outcomes. The findings highlight marked socio-demographic disparities in disease burden and emphasize geographic variations influenced by lifestyle and socio-demographic determinants.
While COI studies predominantly provide descriptive data on the direct and indirect costs of oral cancer, their utility for informing resource allocation remains limited compared to other economic evaluations such as cost-effectiveness analyses. Nevertheless, this review’s detailed cost component delineation across different countries may facilitate future cost-effectiveness studies in oral cancer management and screening programs. The heterogeneity of methodologies among COI studies poses challenges for inter-study comparison, underscoring the World Health Organization’s recommendation to report costs in international dollars adjusted by purchasing power parity (PPP) to enable more accurate cross-country comparisons.
The study also underscores the need for standardized protocols in cost evaluation, similar to those developed by the Pan American Health Organization (PAHO) for hospital infection costs, to reduce heterogeneity and improve the precision of oral cancer cost estimates across various health systems and regions. Observational and randomized controlled trials provided robust evidence of implementation costs and outcomes, whereas modeling approaches offered feasibility for estimating long-term consequences and exploring different strategic options for oral cancer screening and management. Despite these efforts, current evidence regarding the cost-effectiveness of oral cancer screening remains heterogeneous and insufficient to support widespread institutional adoption.
Financial Burden on Patients
Studies assessing the financial burden of mouth cancer on patients have revealed significant out-of-pocket costs (OOPC) that extend beyond direct medical expenses. Most research includes patients undergoing active treatment at various stages, with additional focus on those recently diagnosed, in palliative care, or survivorship phases. Measurement tools for OOPC vary, including patient-maintained cost diaries and logbooks, as well as analyses of health administrative data and insurance claims. These methods capture not only medical expenses but also ancillary and non-medical costs that contribute substantially to the overall financial strain.
The annual out-of-pocket costs borne by mouth cancer patients often encompass expenses for medical supplemental services such as dental care, physiotherapy, and nutrition counseling, which are frequently not covered by insurance. These ancillary services can represent a major source of expenditure, particularly during the treatment and early post-treatment periods, when patients typically face the highest financial burden. Travel and transportation costs also constitute a significant portion of non-medical expenses, especially for patients living in rural or remote areas who must frequently travel for specialized care. Caregiving costs further add to the financial challenges, yet support for these non-medical expenses is inconsistent and varies widely across healthcare systems.
Evidence indicates that the proportion of income spent on out-of-pocket cancer-related costs varies greatly by context and patient demographics. For example, a Canadian study of breast cancer patients estimated that OOPC accounted for approximately 2.3% of household income, whereas in low- and middle-income countries (LMICs), such as India, caregivers of pediatric cancer patients reported incurring debts exceeding 175% of their annual income. Age and ethnicity also influence financial burden; younger adults and patients over 60 years face higher out-of-pocket expenses, while ethnic minorities and indigenous populations often experience greater barriers to care and associated costs.
Beyond the direct financial impact, accumulating out-of-pocket costs can contribute to psychosocial distress among patients and caregivers. Catastrophic health expenditures have been linked to financial strain that may affect treatment adherence and overall quality of life. This underscores the importance of comprehensive cost assessments that include direct medical, direct non-medical, and indirect costs, such as lost income due to illness or caregiving responsibilities. Current research advocates for standardized protocols to better capture these diverse cost components and facilitate comparisons across regions and healthcare systems.
Variations in Cost
The cost of treating mouth cancer varies significantly depending on factors such as the stage of the disease, geographic location, healthcare system infrastructure, and socioeconomic status. Treatment for advanced stages of mouth cancer incurs substantially higher expenses compared to early stages, with unit costs estimated at USD 2,717 for advanced cases versus USD 1,568 for early-stage treatment—a difference of approximately 42%. Furthermore, an increase in socioeconomic status is associated with an 11% reduction in unit costs, highlighting disparities in healthcare access and outcomes.
Geographical variations also play a critical role in cost differences. For instance, in the United States, outpatient care costs often exceed inpatient costs because many patients receive radiotherapy—a notably expensive treatment modality—in outpatient settings. National cost estimates are influenced by cancer prevalence, treatment patterns, and phase of care, with the highest per-patient annualized costs observed during the end-of-life phase (approximately $109,727 for medical services), followed by the initial diagnosis year and continuing care phases. These variations reflect differences in healthcare delivery models and resource allocation across countries.
Indirect costs, such as productivity losses and costs related to premature death, add substantially to the overall economic burden of mouth cancer but are often underreported in studies. Only a subset of research has incorporated early death costs, one of the most expensive components for society. Moreover, disparities in socioeconomic development further influence the incidence, mortality, and disability-adjusted life years (DALYs) associated with lip and oral cavity cancers worldwide, with higher burdens typically observed in lower socio-demographic index regions.
Out-of-pocket expenses and non-reimbursed costs impose additional financial strain on patients and their caregivers, contributing not only to economic hardship but also to psychosocial burdens, including financial distress and potential treatment nonadherence. These pressures affect quality of life and underscore the need for healthcare systems to address cost-related barriers, particularly for vulnerable populations. Overall, the financial impact of mouth cancer is multifaceted, shaped by clinical, economic, and social determinants that create marked variations in cost across different settings.
Treatment Modalities and Their Economic Impact
The treatment of lip and oral cavity cancers involves various modalities, each associated with differing costs and implications for patient care. Surgery remains a common primary treatment; however, radiation therapy is often employed as an alternative, especially for patients who are unable to undergo surgery due to other medical conditions. Radiation is frequently used for cancers located in the floor of the mouth, front of the tongue, inside of the cheek, gums, and hard palate, particularly in cases involving larger tumors, local tissue invasion, or spread to nearby lymph nodes in the neck.
Economic analyses have demonstrated that the costs of treating advanced stages of oral cancers are significantly higher than those for early stages. The unit cost of treating advanced-stage disease was estimated at USD 2,717, representing a 42% increase compared to early-stage treatment costs of USD 1,568. This substantial difference is further highlighted by studies indicating that advanced staging can increase treatment expenses by anywhere from 21.9% to 373.3% relative to early stages, despite variability in clinical staging definitions and tumor locations within the head and neck region. Furthermore, the treatment of recurrent squamous cell carcinoma, particularly in sites such as the floor of the mouth, tongue, and alveolar trigone, was reported to be 51% more expensive over a two-year follow-up compared to primary tumor treatment.
When evaluating the phases of cancer care—initial (first year after diagnosis), continuing, and end-of-life—the highest per-patient annual costs occur during the last year of life. For medical services alone, costs reach approximately $109,727 in this phase, compared to $43,516 during the initial treatment year and $5,518 in the continuing phase. Oral prescription drug costs follow a similar pattern, with $4,372, $1,874, and $1,041 respectively for the same phases. These variations reflect the intensity and complexity of care required at different disease stages.
Patients’ out-of-pocket expenses also contribute to the economic burden and have been assessed using a variety of methods, including cost diaries and health administrative data. Most studies examining these costs focused on patients undergoing active treatment (47%) or those recently diagnosed (24%), with fewer addressing end-of-life care (8%) or survivorship (8%). The comprehensive economic impact underscores the importance of early detection and stage-appropriate treatment strategies, as advanced disease not only leads to poorer health outcomes but also imposes substantially higher financial costs on patients and healthcare systems.
Additionally, socioeconomic factors influence treatment costs; an 11% reduction in unit costs has been observed with increasing socioeconomic status, suggesting disparities in access to or utilization of healthcare resources. Redirecting funds from costly treatments towards screening and early intervention programs may optimize resource allocation and improve overall health outcomes for patients with oral cancers.
Effects of Financial Burden
Cancer patients, particularly those with oral and head and neck cancers, face substantial financial burdens that extend beyond direct medical expenses. Out-of-pocket costs (OOPC) related to treatment, ancillary services, and post-treatment care contribute significantly to the overall economic strain experienced by patients and their families. These costs can lead to catastrophic health expenditures, which not only impose financial hardship but also cause considerable psychosocial distress, adversely affecting patients’ quality of life.
Ancillary services such as dental care, speech therapy, and physical therapy often represent a major source of OOPC during the surveillance and survivorship periods, especially given the complex anatomical and functional challenges associated with head and neck cancer treatments. Despite the clinical necessity of these services, reimbursement policies frequently exclude dental-related care, placing a disproportionate financial responsibility on patients themselves.
The financial toxicity associated with cancer treatment has been linked to nonadherence to prescribed therapies, further complicating health outcomes. Additionally, the economic burden encompasses not only direct healthcare costs but also productivity losses due to morbidity and premature mortality, amplifying the societal impact of oral cancers. Socioeconomic disparities influence the extent of this burden, with lower-income patients often experiencing greater financial and health-related challenges.
Systemic Factors Influencing Costs and Burdens
The financial burden of mouth cancer treatment is shaped by multiple systemic factors that extend beyond direct medical expenses. Health insurance coverage plays a critical role in mitigating the costs of cancer care, yet gaps in coverage or inadequate insurance plans can leave patients vulnerable to high out-of-pocket expenditures. Maintaining continuous and comprehensive health insurance is essential for individuals with cancer to help manage the often unexpected and substantial costs associated with treatment.
Healthcare system structure and resource allocation also significantly impact cost distribution. For example, in the United States, outpatient care costs for oral cancer treatment tend to be higher than inpatient costs due to the prevalent use of radiotherapy in outpatient settings, which is one of the most expensive treatment modalities for mouth cancer management. This variability underscores how the organization and resourcing of healthcare units influence patient expenses.
Non-medical out-of-pocket costs, including transportation, travel, and caregiving expenses, constitute a substantial component of the overall financial burden faced by patients. Support for these non-medical costs is often inconsistent and varies across jurisdictions, exacerbating the economic strain on patients and their families. Such expenditures are essential to enable access to and continuation of cancer treatment but frequently remain inadequately
Responses and Recommendations
Efforts to address the financial burden of mouth cancer treatment have emphasized the importance of early detection and standardized cost evaluations. Early-stage detection through routine oral inspections during dental visits and integration into primary care significantly improves survival rates, with early-stage lesions showing approximately 80% five-year survival compared to 50% or less for advanced stages. To support this, targeted educational programs for high-risk populations and primary care providers are recommended to increase awareness of early signs and symptoms.
Standardizing cost reporting is also critical for improving the comparability of economic studies on oral cancer. The World Health Organization (WHO) advocates for reporting costs in international dollars based on purchasing power parity (PPP) to facilitate cross-country comparisons. Additionally, development and adoption of cost evaluation protocols, similar to those implemented by the Pan American Health Organization (PAHO) for hospital infections, are encouraged to reduce heterogeneity in cost assessments and improve accuracy.
Addressing the financial toxicity faced by patients extends beyond medical expenses. Studies highlight substantial out-of-pocket costs related to ancillary services such as dental care, speech therapy, and physical therapy, which are especially prominent in head and neck cancer patients due to the complexity of treatment and survivorship needs. Non-medical expenses, including transportation and caregiving, also contribute significantly to the overall financial burden, yet support for these costs remains inconsistent across health systems. These financial strains can lead to psychosocial distress and reduced quality of life, underscoring the need for comprehensive financial support mechanisms.
To mitigate these issues, policymakers and healthcare providers are encouraged to develop integrated care models that include financial counseling, coverage of ancillary services, and support for non-medical costs. Moreover, increasing access to regular dental visits and reducing out-of-pocket dental expenses can lower the financial barriers to care, as patients with higher educational attainment, income, and pre-treatment dental visits are less likely to experience financial hardship related to mouth cancer treatment.
Criticisms and Limitations
Despite providing valuable insights into the economic burden of oral cancer, the reviewed studies exhibit several notable criticisms and limitations. One key issue is the limited utility of cost-of-illness (COI) analyses in guiding resource allocation compared to other health economic evaluations such as cost-effectiveness analyses. Many studies failed to comprehensively include all relevant cost components, with only one out of 24 reviewed studies considering all components of COI simultaneously. Moreover, among the few that analyzed indirect costs, only half included costs related to early death from oral cancer—an especially significant societal expense. These gaps suggest that the overall costs are likely underestimated, emphasizing the need for more methodologically rigorous and longitudinal studies with improved data analysis and reporting standards.
Inter-study comparisons remain challenging due to substantial variability in study design and methodology. While observational and randomized controlled trials tend to provide more accurate evidence regarding implementation costs and outcomes, modeling approaches are often used to estimate long-term consequences and explore different strategy options. However, current evidence on the cost-effectiveness of oral cancer screening is heterogeneous and insufficient to support widespread institutional adoption.
Another critical limitation relates to the treatment of non-medical out-of-pocket costs such as transportation, travel, and caregiving expenses. These costs, which are essential for accessing and utilizing cancer treatment, are inconsistently supported across different healthcare systems. This inconsistency contributes significantly to the overall financial burden experienced by patients. Importantly, medical debt is not confined to low- and middle-income countries; it also affects insured individuals in high-income countries due to the rising costs of novel therapies and strained healthcare resources. Consequently, better characterization and comparison of out-of-pocket burdens across settings are necessary to identify at-risk populations and understand the specific expenses that most heavily impact patients.
The content is provided by Sierra Knightley, Lifelong Health Tips