Summary
Mouth cancer, also known as oral cancer, refers to malignant tumors that develop in the tissues of the mouth, including the lips, tongue, cheeks, gums, and palate. It is a significant global health concern due to its high morbidity and mortality rates, particularly in regions where risk factors such as tobacco use, betel quid chewing, and excessive alcohol consumption are prevalent. Early detection is critical for improving patient outcomes, yet oral cancer often presents with subtle or nonspecific symptoms, leading to delayed diagnosis.
The incidence of mouth cancer varies widely worldwide, with the highest burden observed in South and Southeast Asia, where cultural practices like betel quid chewing combined with tobacco use substantially elevate risk. Other regions, including parts of Eastern Europe and South America, also report elevated rates linked primarily to tobacco and alcohol use. Meanwhile, some Western countries have seen stabilization or declines in traditional oral cancer cases, although infections with human papillomavirus (HPV) are contributing to a rising subset of oropharyngeal cancers. Demographic factors such as age, sex, socioeconomic status, and ethnicity further influence disease patterns and survival outcomes.
Key early warning signs of mouth cancer include persistent white or red patches, non-healing sores, lumps, bleeding, and difficulty with oral functions such as chewing or speaking. Because these symptoms can mimic benign conditions, professional evaluation through clinical examination, imaging, and biopsy is essential for accurate diagnosis. Treatment strategies commonly involve surgical tumor removal, often combined with radiotherapy and chemotherapy depending on the stage and extent of disease, with reconstructive surgery playing a crucial role in restoring function and appearance.
Prevention efforts focus on reducing exposure to known risk factors, including tobacco, areca nut products, and alcohol, alongside public health initiatives promoting early detection and HPV vaccination where applicable. Despite advances in diagnosis and treatment, mouth cancer remains a major challenge worldwide, especially in low- and middle-income countries where access to care and awareness are limited, underscoring the need for comprehensive global action to reduce its burden.
Overview
Oral cancer, commonly referred to as mouth cancer, encompasses malignant growths affecting the inside of the mouth. It often manifests as white patches or sores that bleed and do not heal, distinguishing it from benign oral conditions. Early detection remains the most effective strategy to reduce morbidity and mortality associated with oral cancer, though this requires improved awareness and changes in public and professional practices.
Globally, the incidence of oral cancer varies significantly by region, largely influenced by cultural habits and risk factors such as tobacco use, betel quid chewing, and alcohol consumption. Countries in South Asia, including India, Sri Lanka, Pakistan, and Bangladesh, experience disproportionately high rates due to widespread betel quid chewing often combined with tobacco. Other regions with elevated oral cancer rates include parts of Eastern Europe and South America, where tobacco and alcohol use are prevalent. Conversely, some Western countries have reported stabilization or declines in certain oral cancer types, although those linked to human papillomavirus (HPV) are on the rise.
Age-standardized rates (ASRs) are used to compare oral cancer incidence across populations with different age structures, as age significantly influences cancer risk. However, a high ASR does not always translate into a large number of cases and vice versa, depending on the size of the population. Understanding these statistics helps identify high-risk regions and populations, guiding targeted public health interventions.
Efforts to combat oral cancer include global initiatives such as the World Health Organization’s Global Oral Health Action Plan 2023–2030, which emphasizes regulating smokeless tobacco and areca nut use, particularly in high-burden countries. Diagnosis is increasingly refined through immunohistochemical techniques and specialized imaging like CT scans and MRIs, aiding precise cancer identification and treatment planning. Surgical interventions, ranging from curative tumor removal to reconstructive procedures, play a central role in treatment.
Risk Factors and Etiology
Oral cavity and oropharyngeal cancers are influenced by a variety of risk factors that increase an individual’s likelihood of developing these diseases. Tobacco use, in both smoking and smokeless forms, is the predominant risk factor, accounting for approximately 85% of oral cancer cases globally. The risk escalates with the duration and frequency of tobacco consumption. Smoking is primarily associated with cancers of the mouth and throat, while smokeless tobacco products, such as naswar—which is placed in the buccal sulcus and absorbed through the oral mucosa—have been identified as carcinogenic agents by the World Health Organization, although some controversy regarding their exact role in carcinogenesis remains.
Alcohol consumption also plays a significant role, often acting synergistically with tobacco to increase oral cancer risk. This combination notably raises susceptibility, particularly in East Asian populations, where both smoking and alcohol use are prevalent. Involuntary (secondhand) smoking has additionally been implicated as a risk factor in certain demographics. Other behavioral and environmental exposures, such as prolonged sunlight exposure or use of sunbeds, may contribute to cancers affecting the lips.
Certain infectious agents have a recognized etiological role, most notably human papillomavirus (HPV), especially the HPV16 subtype. HPV-associated oropharyngeal cancers form a distinct clinicopathological entity characterized by a higher prevalence in males, better prognosis, and a lower association with traditional risk factors such as heavy tobacco and alcohol use. HPV-related cancers primarily affect the oropharynx, including the base of the tongue and tonsillar regions, and are less commonly implicated in anterior oral cavity cancers.
Demographic factors such as age and sex also influence risk. Oral cancer incidence is higher in individuals over 40 years of age and shows a male predominance, with white males being more affected than black males in oropharyngeal cancer cases. Socioeconomic determinants—including income, education, and access to healthcare—further impact disease prevalence and outcomes, especially in low- and middle-income countries where tobacco use remains high and tobacco control measures are often insufficiently implemented.
Other less common but notable risk factors include immune system suppression due to medications or diseases, and certain chronic conditions such as severe lichen planus, which may elevate the risk of malignant transformation in oral tissues. Genetic predispositions may also contribute to oral cancer susceptibility, with approximately 10% of all cancers having a strong hereditary component, although research in this area is ongoing.
Understanding these diverse risk factors is crucial for prevention strategies, early detection, and reducing the global burden of oral cancers, particularly in regions with high prevalence linked to cultural practices such as betel quid chewing combined with tobacco use.
Demographics and Populations at Risk
Oral cancer exhibits significant demographic and geographic variations in incidence and outcomes, influenced by socioeconomic, cultural, and lifestyle factors. A notably high prevalence has been observed in South and Southeast Asia, with India alone accounting for approximately one-third of the global burden of oral cancer. Countries such as Sri Lanka, Pakistan, and Bangladesh also bear a disproportionate burden largely due to the widespread cultural practice of betel quid chewing, often combined with tobacco use. Additionally, parts of Eastern Europe and South America report elevated rates, primarily driven by high tobacco and alcohol consumption.
Socioeconomic status plays a critical role in the disease burden. Developing countries generally experience more severe impacts from oral cancer compared to developed nations, with low socioeconomic status itself contributing to an increased risk comparable to traditional lifestyle factors like tobacco and alcohol use. This disparity is further underscored by the negative correlation between oral cancer burden and the Socio-demographic Index (SDI), indicating that countries with lower economic development face disproportionate challenges relative to their economic resources.
Gender differences are also prominent in oral cancer demographics. Historically, the disease has been more common in males, with a male-to-female ratio of approximately 4:1 in oropharyngeal cancers, though this has shifted closer to 2:1 in cancers of the anterior mouth, likely reflecting increased tobacco use among women in recent decades. Racial disparities exist as well; for instance, oral cancer incidence and mortality rates are higher in Black populations compared to Whites in the United States, with five-year survival rates reported at 33% for Blacks versus 55% for Whites. Despite these disparities, some trends show improvement, such as a significant decline in oral cancer incidence rates among Black individuals over the past 30 years.
Age is a well-recognized risk factor, with oral cancer most frequently occurring in individuals over 40 years old. Overall, while age, gender, race, socioeconomic status, and regional lifestyle practices influence oral cancer risk, the interplay of these factors creates complex patterns of incidence and survival across different populations worldwide.
Early Warning Signs and Symptoms
Oral cancer can develop in various parts of the mouth, including the lips, inner lining of the cheeks, salivary glands, gums, tongue, hard palate, and soft palate. Because of its diverse locations, early signs and symptoms may vary and are often subtle, making early detection challenging.
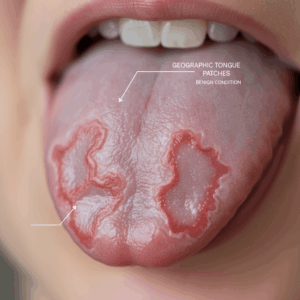
One of the earliest indications can be the appearance of white patches (leukoplakia) or red patches (erythroplakia) on the tongue or inside the mouth. Erythroplakia presents as bright red, velvety plaques that cannot be clinically or pathologically classified as any other condition and is considered a significant risk marker for malignancy. White patches, though common and sometimes caused by other non-cancerous conditions, should be evaluated carefully by a dentist or physician, especially if persistent.
Other early symptoms may include ulcers, lumps, or pain inside the mouth. A lesion that bleeds during routine activities such as tooth brushing, even if the bleeding is minimal, can be an early warning sign. However, continuous or heavy bleeding is less typical in early oral cancer and may suggest advanced disease or other conditions. Rough or crusty areas on the lips, gums, or inside the mouth, as well as numbness, pain, or tenderness on the face, neck, or inside the mouth without apparent cause, should also raise suspicion.
Difficulty with oral functions such as chewing, swallowing, speaking, or moving the jaw or tongue may occur as the cancer progresses. This can be accompanied by symptoms like chronic bad breath and unintentional weight loss. In some cases, involvement of nerves can cause hypersensitivity or pain, and invasion of the jaw muscles or bone may lead to trismus (lockjaw), significantly restricting mouth opening.
Due to the subtlety of these symptoms and their overlap with less serious conditions, professional examination is crucial. Dentists and general practitioners will usually perform a thorough oral examination, including inspection and palpation of the mouth, neck, and jaw, and may recommend further diagnostic tests such as biopsies for any suspicious lesions. Early recognition and evaluation of these warning signs improve the chances of successful treatment and better outcomes.
Diagnosis
Diagnosing mouth cancer involves a combination of clinical examination, imaging studies, and biopsy procedures to confirm the presence and extent of the disease. Early detection is crucial for improving outcomes, yet mouth cancer often shows no symptoms in its initial stages, making thorough screening essential, especially for individuals at higher risk such as tobacco and alcohol users.
Clinical Examination and Imaging
The diagnostic process typically begins with a detailed history and physical examination, including visual inspection and palpation of the head, neck, oral, and pharyngeal regions. Digital palpation of lymph nodes, bimanual palpation of the floor of the mouth and tongue, and inspection of oral and pharyngeal mucosa with adequate lighting and tools like mouth mirrors are standard components of the exam.
Advanced imaging technologies such as CT scans, MRIs, and specialized X-rays (e.g., Panorex) help define the precise extent of tumors and guide biopsy decisions. Positron emission tomography (PET) combined with CT may be utilized to detect metastatic spread to lymph nodes or other body parts. For lesions located deep within the mouth or throat, imaging also assists in planning biopsy procedures that may require general anesthesia.
Biopsy Procedures
A biopsy is the definitive diagnostic test for confirming mouth cancer. The most common type is the incisional biopsy, where a small piece of suspicious tissue is surgically removed and examined microscopically for cancer cells. For tumors located deeper in the oral cavity or oropharynx, the biopsy may be performed under general anesthesia in an operating room to ensure patient comfort and adequate tissue sampling.
Fine needle aspiration (FNA) biopsy, which involves extracting cells with a thin hollow needle, is primarily used to sample neck lumps or masses rather than oral lesions directly. It is especially useful for evaluating suspected metastatic lymph nodes or salivary gland tumors. However, FNA is not suitable for initial diagnosis of oral mucosal abnormalities.
Adjunctive Diagnostic Tests
In addition to traditional biopsy, several adjunctive tests assist in identifying suspicious lesions or monitoring patients with a history of oral cancer or potentially malignant disorders (PMD). These include vital staining with dyes such as toluidine blue, cytology, and the use of fluorescent light or fluorescent mouthwashes to differentiate abnormal tissue from healthy mucosa.
Although these adjunctive methods can enhance detection and help in selecting biopsy sites, none currently replace the gold standard of surgical biopsy with histological examination. Cytology, in particular, shows promise due to its relatively high sensitivity and specificity and may be valuable when combined with other tests.
Prevention Strategies
Preventing mouth cancer involves a combination of lifestyle modifications, early detection, and targeted interventions, particularly in high-risk populations. One of the most effective measures to significantly reduce the risk of oral cancer is avoiding or quitting tobacco use, including smoking and the consumption of areca nut products such as betel quid, with or without tobacco. Additionally, reducing alcohol intake plays a crucial role in lowering the risk. The World Health Organization has identified smokeless tobacco as a carcinogen, and its use, such as in the form of naswar, contributes to oral cancer risk through absorption of harmful agents via the oral mucosa.
Early detection programs targeting populations with high incidence rates—especially in South and South-East Asia and the Western Pacific islands—are vital to decreasing the incidence and mortality of advanced oral cancer stages. Routine dental check-ups that include comprehensive oral examinations can facilitate early identification of oral cancers and potentially malignant disorders (PMDs). Dentists often perform brief oral cancer screenings during regular visits, inspecting the mouth, lips, face, and neck for suspicious signs. Techniques such as fluorescent light examination may also aid in early detection.
Reducing exposure to risk factors remains essential, as changes in lifestyle and risk factor prevalence have influenced oral cancer trends, particularly in high-income countries. However, low- and middle-income countries face significant challenges due to poor public awareness of risk factors and difficulties implementing tobacco control policies, which may lead to increasing oral cancer burdens in these regions. In addition to tobacco and alcohol, human papillomavirus (HPV) infection is recognized as an important risk factor for a subset of oral cancers. While HPV-related oral cancers typically occur in individuals without heavy tobacco or alcohol use and tend to have a better prognosis, prevention efforts such as HPV vaccination may contribute to reducing incidence rates.
Treatment
Treatment of mouth cancer depends on the type, size, location, and stage of the tumor, as well as the patient’s overall health. Surgery is the most common initial treatment for oral cancers and aims to remove the tumor completely while preserving as much normal tissue and function as possible. For smaller or early-stage lesions, surgical resection alone may be sufficient, often followed by reconstructive surgery to restore appearance and function. Larger or deeper tumors, especially those that have spread to lymph nodes in the neck, typically require more extensive surgery, which may include lymph node dissection to check for cancer spread.
Radiation therapy is frequently used either as a primary treatment or postoperatively to target residual cancer cells. It may be chosen instead of surgery for patients who are not good candidates for surgery due to other medical issues. Radiation can also be combined with chemotherapy (
Prognosis and Survival Rates
The prognosis and survival rates for mouth cancer depend heavily on several factors, including the stage at diagnosis, the type of cancer, and the patient’s overall health. Early detection and treatment are critical, as early-stage mouth cancers (stage I and II) generally have a better prognosis compared to more advanced stages. Treatment goals may vary between aiming for a cure or managing symptoms to improve quality of life, and understanding these goals can help patients weigh the risks and benefits of different treatment options.
Survival rates also differ based on socioeconomic and demographic factors. The burden of oral cancer is disproportionately higher in low-income countries, where access to timely diagnosis and effective treatment may be limited, negatively impacting survival outcomes. Furthermore, epidemiological data show significant regional variations in the incidence and mortality of mouth cancer, often linked to lifestyle and environmental factors.
Age is a known risk factor influencing prognosis, with most cases occurring in individuals over 40 years old, and the disease tends to be more common among males, particularly white males, than females. Standardized incidence rates (ASRs) are used to compare the disease burden across populations with differing age structures, revealing that countries with either high or low ASRs may have vastly different total case numbers depending on their population size.
When to Seek Medical Advice
It is important to seek medical advice if you experience symptoms that could indicate mouth cancer, especially if they persist for more than two weeks. Common warning signs include sores, irritations, or unusual thickness in the mouth or throat that do not heal within this time frame. While having these symptoms does not definitively mean you have mouth cancer, prompt evaluation by a general practitioner (GP) or dentist is essential for early detection and diagnosis.
During the examination, the healthcare professional will typically inspect and feel inside your mouth, as well as check your neck and jaw for any abnormalities. You have the right to request that someone else be present during the examination for support or reassurance. If the GP suspects the presence of cancerous symptoms, you may be given an urgent referral for further testing or to see a specialist in a hospital setting.
Early detection remains the most effective strategy to reduce morbidity and mortality from oral cancer. Therefore, it is crucial to be vigilant about any persistent oral symptoms and seek timely medical attention to improve treatment outcomes.
Resources and Support
Numerous resources are available to support individuals affected by mouth cancer, ranging from population-based data to clinical guidance and patient-centered care. The International Agency for Research on Cancer (IARC) compiles data from global cancer registries through projects such as Cancer Incidence in Five Continents and GLOBOCAN, providing critical epidemiological information that informs prevention and treatment strategies worldwide.
In alignment with global health initiatives, the World Health Organization (WHO) has developed the Global Oral Health Action Plan 2023–2030, which includes a comprehensive Handbook aimed at regulating the use of smokeless tobacco and areca nut—both significant risk factors in countries with high oral cancer rates. This resource serves as a key tool for policymakers and health professionals working to reduce the burden of oral cancers.
For patients undergoing treatment, it is essential to maintain open communication with healthcare providers to understand the goals of therapy, whether curative or palliative, and to weigh the risks and benefits of different options. Multidisciplinary teams, including oncologists and certified oncology nurses, are involved in delivering tailored cancer care and supporting patients throughout their journey. Moreover, involving patients in decision-making processes is critical, particularly in complex clinical scenarios such as early postoperative recurrence or planning adjuvant therapies. Emerging evidence from sentinel lymph node biopsy trials supports personalized neck management approaches in oral cavity cancer, emphasizing the importance of individualized treatment plans.
Diagnostic and monitoring tools also play a crucial role in managing oral cancer. Various tests and examinations aid in detecting oral cancers and monitoring patients with a history of the disease or potentially malignant disorders (PMD). However, factors such as patient selection and the complexity of mucosal changes after prior treatments can influence diagnostic accuracy. Adjunctive tests like the Conventional Oral Examination (COE) have been studied for early detection of PMD and remain a foundational step in clinical assessment.
Collectively, these resources and support systems—from global data initiatives and policy frameworks to patient-centered clinical care and diagnostic advancements—are vital for improving outcomes and quality of life for those affected by mouth cancer.
The content is provided by Avery Redwood, Lifelong Health Tips