Summary
Discover Early Warning Signs of Mouth Cancer on World Cancer Day
Mouth cancer, also known as oral cancer, encompasses malignant tumors that develop in the tissues of the mouth and throat. Ranking as the 16th most common cancer globally, it poses a significant public health challenge due to its often subtle early symptoms and potential for rapid progression if untreated. Early warning signs such as persistent white or red patches (leukoplakia and erythroplakia), non-healing ulcers, lumps, or unexplained bleeding in the oral cavity can easily be mistaken for benign conditions, leading to delays in diagnosis and treatment. Human papillomavirus (HPV), particularly high-risk strains like HPV-16, has emerged as a notable cause of oropharyngeal cancers, which may lack obvious mucosal lesions, complicating early detection efforts.
World Cancer Day serves as a global platform to increase awareness about mouth cancer, emphasizing the critical role of recognizing early warning signs to facilitate timely diagnosis and improve treatment outcomes. Numerous countries coordinate awareness campaigns and screening initiatives on this day to educate high-risk populations—such as tobacco and alcohol users—on self-examination techniques and encourage regular clinical screenings. These efforts aim to reduce the global burden of oral cancer by promoting early identification of premalignant lesions, which can transform into invasive cancers if left unaddressed.
Early detection methods include visual and tactile oral examinations performed by healthcare providers, supplemented by adjunctive tools such as toluidine blue staining, which helps highlight dysplastic or malignant cells. Definitive diagnosis relies on biopsy and histopathological evaluation, with molecular studies increasingly aiding risk stratification by identifying genetic alterations linked to malignant progression. Despite available educational resources for clinicians, the uptake and efficacy of early detection programs remain inconsistent, underscoring the need for expanded public and professional training.
Recognizing and addressing the early signs of mouth cancer on World Cancer Day highlights the importance of public education, targeted screening, and prevention strategies, including tobacco cessation and HPV vaccination. By fostering greater awareness and prompt medical evaluation of suspicious oral changes, these initiatives strive to improve survival rates and reduce the morbidity associated with this potentially fatal disease.
Background
Mouth cancer, also known as oral cancer, refers to malignant growths that affect the tissues inside the mouth and throat. It is the 16th most common cancer worldwide. The disease can be life-threatening if left untreated and often manifests as changes that may initially resemble common oral issues such as white patches or sores that bleed. Unlike typical oral irritations, these changes do not resolve over time, signaling potential malignancy.
Early morphological changes associated with oral cancer include the development of premalignant lesions such as leukoplakia and erythroplakia. Leukoplakia presents as a white plaque that cannot be removed by gentle scraping and lacks an identifiable cause. Genetic alterations have been demonstrated in these premalignant lesions, suggesting their role in the progression to cancer.
Staging of oral cancer is commonly described using terms like local, regional, or distant. Local stage indicates that the cancer is confined to the mouth, regional denotes spread to cervical lymph nodes in the neck, and distant refers to metastasis to areas far from the oral cavity.
One significant challenge in early detection is the increasing incidence of oral cancers caused by the human papillomavirus (HPV16), particularly in the oropharynx, tonsils, and base of the tongue. These HPV-related cancers often do not produce visible lesions or discolorations, which have traditionally served as early warning signs for cancers located in the anterior parts of the mouth.
Despite the availability of educational materials aimed at healthcare providers to improve early detection, their use remains limited and the effectiveness of these resources has yet to be fully assessed. Additionally, screening methods require validation against gold standards, such as expert clinical or histopathological diagnosis, to ensure accurate identification of true positive and negative cases.
World Cancer Day
World Cancer Day serves as a global platform to raise awareness about various types of cancer, including mouth cancer, and emphasizes the importance of early detection and prevention. It aims to engage the public and healthcare professionals in recognizing early warning signs of mouth cancer, thereby promoting timely diagnosis and improved treatment outcomes.
In many countries, awareness campaigns are organized around this day to educate high-risk populations on self-examination techniques and to encourage regular screenings. For example, in India, targeted efforts include screening of individuals at high risk, promoting oral self-examination, and involving village health workers to facilitate early detection and awareness of head and neck cancers. Similarly, several nations observe national mouth cancer awareness days or weeks in conjunction with World Cancer Day, using various outreach methodologies to reach diverse audiences and healthcare providers.
Given that mouth and oral cancer ranks as the 16th most common cancer worldwide, these awareness initiatives are critical in addressing its global burden. Early identification of premalignant lesions such as leukoplakia and carcinoma in situ is essential since these conditions can progress to invasive oral cancers if left untreated. Thus, World Cancer Day functions not only to highlight the impact of mouth cancer but also to disseminate knowledge on prevention, risk factors, and early signs that can significantly reduce mortality and morbidity associated with this disease.
Early Warning Signs of Mouth Cancer
Mouth cancer can present with a variety of early warning signs that are often subtle and easily mistaken for less serious conditions. Recognizing these signs is crucial for early detection and improved treatment outcomes.
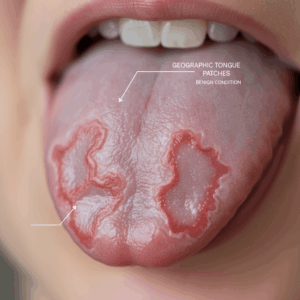
One of the most common early indicators is the appearance of white patches on the tongue or inside the mouth, which cannot be scraped off. These white plaques, often referred to as leukoplakia, are considered premalignant lesions and warrant further investigation. Similarly, red patches (erythroplakia) may also signal premalignant changes. These lesions are typically painless but can vary in appearance, making clinical diagnosis challenging without histopathologic confirmation.
Early mouth cancer may also present as mouth ulcers that do not heal, lumps, or persistent patches inside the cheeks, gums, lips, or on the tongue. In some cases, patients might notice small amounts of blood mixed with saliva during brushing, although continuous or heavy bleeding is less common and may indicate advanced disease. Other symptoms can include numbness, pain, or difficulty moving the tongue or swallowing. Changes in denture fit, a sore throat, hoarseness, or a persistent earache may also be associated with oral cancer or related oropharyngeal cancers.
As the disease progresses, involvement of the jaw muscles or bone can lead to trismus, or lockjaw, limiting mouth opening. Additionally, the presence of a lump in the neck could signify lymph node metastasis, an indicator of more advanced disease.
Because these symptoms often mimic common oral conditions, it is important to consult a healthcare professional if any suspicious signs persist beyond two weeks. Dentists and general practitioners can perform oral examinations, palpate the floor of the mouth, and check for neck masses. Suspicious lesions may be further evaluated with biopsies or adjunctive diagnostic tools such as toluidine blue staining, which helps identify dysplastic or malignant cells by selective dye uptake.
Early detection of mouth cancer improves prognosis significantly, emphasizing the importance of awareness and prompt medical consultation when these warning signs appear.
Risk Factors and High-Risk Populations
Oral cancer risk is influenced by multiple factors, with tobacco and alcohol use being the most significant contributors. Approximately 85 percent of patients with oral cancers have a history of tobacco use, including cigarettes, chewing tobacco, or snuff. The risk increases with the duration and frequency of use, affecting different areas such as the mouth, throat, cheeks, gums, and inner lips depending on the form of tobacco consumed. Additionally, populations that use both tobacco and alcohol have a 10 to 30 times higher risk of developing a second head and neck malignancy compared to the general population. Due to this elevated risk, early detection is critical to reducing morbidity and mortality associated with oral cancer.
Human papillomavirus (HPV) infection is another important risk factor, particularly for oropharyngeal cancers. High-risk HPV types, especially HPV-16 and HPV-18, have been linked to oral potentially malignant disorders and squamous cell carcinoma of the oral cavity. HPV-related oral cancers typically occur in individuals who are not tobacco or alcohol users and generally have a better prognosis. While HPV is definitively implicated in oropharyngeal cancers affecting areas such as the base of the tongue and tonsils, its role in anterior mouth cancers is less common but still notable.
Certain genetic conditions greatly increase susceptibility to oral cancer. For example, individuals with Fanconi anemia face up to a 500-fold higher risk compared to the general population. Dyskeratosis congenita, another inherited syndrome, also confers a high risk of early-onset oral cancer.
Betel nut chewing has been associated with the development of oral premalignant lesions such as leukoplakia, alongside cigarette smoking, tobacco, and alcohol exposure. Given the varied appearance of premalignant lesions, histopathologic diagnosis remains more reliable than clinical examination alone for assessing malignant potential.
Because tobacco and alcohol use also elevate the risk of cancers in the esophagus and lung, there is up to a 10% chance of concurrent malignancies in these regions among oral cancer patients. This necessitates thorough examinations such as panendoscopy to rule out additional cancers.
Methods of Early Detection and Diagnosis
Early detection of mouth cancer is crucial for improving prognosis and survival rates. The initial morphologic changes often present as premalignant lesions, such as leukoplakia—a white plaque that cannot be removed by gentle scraping and lacks other identifiable causes—and erythroplakia. Genetic alterations have been demonstrated in these lesions, highlighting their potential for malignant transformation.
Oral cancer screening plays a vital role in identifying early signs of malignancy. During a screening, healthcare providers conduct a thorough visual and physical examination of the entire oral cavity, including the gums, tongue, lips, cheek lining, tonsils, and roof of the mouth. Palpation of the neck, floor of the mouth, and tongue is also performed to detect any abnormalities. These screenings are typically brief, often lasting less than five minutes, and may involve the use of oral screening dyes or special light sources to highlight suspicious areas.
If a suspicious lesion is identified during screening, a biopsy is the definitive diagnostic method. A tissue sample is taken from the abnormal area and examined histopathologically to confirm malignancy or premalignant changes. Prompt biopsy is essential to avoid delays in diagnosis and treatment. In some cases, healthcare providers may recommend follow-up visits to monitor lesion progression or resolution before proceeding with invasive procedures.
Adjunctive tools such as toluidine blue staining can aid in the detection process. This vital dye selectively binds to dysplastic or malignant cells due to their increased DNA content and acidic tissue components, thereby helping to delineate abnormal tissue during clinical examination. Its simplicity, low cost, and noninvasive nature make it a valuable complement to visual inspection and biopsy planning.
Advanced imaging techniques, including computed tomography (CT) and magnetic resonance imaging (MRI), are frequently used for staging oral cancers and assessing the extent of disease. However, their utility in early detection is limited by the small size of initial lesions. Ongoing improvements in imaging resolution and molecular diagnostic methods hold promise for better identification of nasopharyngeal, submucosal, and bone involvement at earlier stages.
Public education on oral self-examination is another preventive strategy that can increase awareness and prompt earlier professional evaluation. Although self-examinations should not replace clinical screening, they serve as a secondary measure to identify early lip and mouth lesions. Educational programs targeting both healthcare professionals and the general population have shown some effectiveness in improving early detection rates, though wider implementation and evaluation are needed.
Histopathological and Molecular Features
Oral premalignant lesions (OPLs) exhibit a wide range of appearances that challenge straightforward clinical classification, often necessitating histopathological examination for accurate diagnosis and assessment of malignant potential. Histologically, these lesions may show hyperkeratosis, various degrees of epithelial dysplasia, carcinoma in situ (CIS), or invasive squamous cell carcinoma. Despite this, there is often no direct correlation between the macroscopic morphology of the lesion and its histopathological grade.
The progression of oral cancer typically follows a histopathological continuum beginning with mild (low-grade) dysplasia, advancing through moderate and severe (high-grade) dysplasia, then carcinoma in situ, and ultimately invasive disease. Approximately 5–18% of epithelial dysplasias undergo malignant transformation, though establishing a definitive relationship between the degree of dysplasia and the risk of malignancy remains complex due to limitations in longitudinal observation of untreated lesions. Early detection of OPLs with a high likelihood of progression is essential for effective cancer prevention and management.
At the molecular level, genomic instability plays a central role in the malignant transformation of oral premalignant lesions. This instability manifests as alterations in ploidy, changes in DNA content, copy number variations, loss of heterozygosity, and mutations in key cancer driver genes. One of the most frequently mutated genes in oral premalignant lesions is TP53, a tumor suppressor gene whose mutation is strongly associated with progression to invasive carcinoma. Approximately 50% of head and neck cancers, including those originating in premalignant lesions, harbor TP53 mutations.
Copy number alterations in NOTCH1 have also been implicated in the transition from premalignancy to invasive oral cancer. Loss of NOTCH1 function induces expression of matrix metalloproteinases, cytokines, and chemokines that remodel the tumor microenvironment, promoting tumor progression and altering immune cell infiltration. Changes in the tumor microenvironment driven by such molecular alterations contribute to the immunosuppressive milieu observed in oral premalignant lesions, impacting immune cell recruitment including macrophages and dendritic cells.
The development of oral cancer is commonly linked to exposure to carcinogens such as tobacco and alcohol, which initiate molecular changes in the mucosal epithelium. These changes set in motion a cascade of genetic and epigenetic events leading to genomic instability and eventual malignant transformation. Consequently, molecular assessment of premalignant lesions offers a promising approach to improve risk stratification beyond traditional histopathological methods, as genomic alterations have been shown to better predict progression in low-grade dysplasias.
Staging Systems for Mouth Cancer
Staging of mouth cancer is a critical step following diagnosis, as it helps determine the extent of the disease and guides treatment decisions. The process, known as staging, evaluates whether the cancer has spread and how far, considering factors such as tumor size, involvement of lymph nodes, and distant metastasis.
The most widely accepted method for staging mouth cancer is the tumor-node-metastasis (TNM) classification system. This system assesses three main clinical features: the size of the primary tumor measured in centimeters, the presence and extent of spread to local lymph nodes—including number, size, and whether the spread is unilateral or bilateral—and the existence or absence of distant metastasis. For example, stage 1 mouth cancer corresponds to a tumor that is 2 cm or smaller and 5 mm deep or less, with no spread to nearby tissues, lymph nodes, or other organs. In TNM terms, this is classified as T1, N0, M0.
Mouth cancer is generally classified into five stages, from stage 0 to stage IV, with stage IV representing the most advanced disease. The initial staging is typically assigned after a physical examination and preliminary biopsy or imaging tests. However, the stage may be updated following further diagnostic procedures or surgery.
While imaging techniques such as CT scans and MRIs are commonly used to aid staging, they may not always fully capture the anatomical details necessary for precise staging, sometimes necessitating repeat studies. Additionally, due to the phenomenon of “field cancerization” in the head and neck region, patients diagnosed with primary squamous cell carcinoma or epithelial dysplasia of the oral cavity should be evaluated for synchronous tumors.
Accurate staging is essential as tumor size, affected tissues, and the extent of spread are among the best indicators of patient prognosis and guide therapeutic approaches.
Awareness Campaigns and Screening Programs on World Cancer Day
Raising public awareness and promoting early detection through screening are crucial strategies in improving outcomes for patients with mouth cancer. Awareness campaigns, particularly those timed with global observances such as World Cancer Day, play an essential role in educating the public about the signs, symptoms, and risk factors associated with oral cancer, including tobacco use, alcohol consumption, and human papillomavirus (HPV) infection.
Various countries have implemented targeted campaigns aimed at increasing awareness and encouraging early diagnosis. For example, in India, efforts focus on screening high-risk individuals, promoting oral self-examination, and engaging village health workers to enhance early detection and public knowledge of head and neck cancers. Similarly, several nations have established national mouth cancer awareness days or weeks that mobilize primary healthcare professionals and the public through diverse methodologies to facilitate earlier presentation and diagnosis.
Screening programs are a key component of these campaigns. Although screening tests for oral cancer are not diagnostic, they serve to identify individuals with abnormal oral findings who require further evaluation by specialists such as oral and maxillofacial surgeons or ear, nose, and throat (ENT) experts. An effective screening program depends on multiple factors including high participation rates, proper training and calibration of screeners, quality control of screening procedures, and a clear referral pathway to ensure timely diagnosis and treatment.
Educational interventions extend beyond healthcare providers to the general population, encouraging oral self-examination as a supplementary preventive measure. Self-examinations help individuals become familiar with their oral cavity and potentially identify early lesions, although they should complement, not replace, professional screenings. Despite the availability of educational resources for clinicians, their utilization and impact on early detection remain limited, underscoring the need for expanded and evaluated training programs.
Prevention and Risk Reduction Strategies
Early detection and prevention are crucial in improving survival rates for oral cancer. Low public awareness and delays in seeking medical attention for symptoms have been identified as significant factors contributing to poor outcomes, highlighting the need for enhanced public education campaigns to promote earlier diagnosis and treatment. Raising awareness about oral cancer signs and symptoms, as well as encouraging regular dental check-ups, plays a vital role in early screening and detection.
Tobacco use remains the primary risk factor for oral cancer, with approximately 85% of patients reporting tobacco consumption in forms such as cigarettes, chewing tobacco, or snuff. The risk correlates with the duration and frequency of tobacco exposure. Alcohol consumption also significantly increases the risk, and combined use of tobacco and alcohol further exacerbates this effect. Additionally, betel nut chewing has been linked to premalignant oral lesions such as leukoplakia.
Human papillomavirus (HPV) infection, particularly with high-risk types HPV-16 and HPV-18, has emerged as an important etiological factor for oropharyngeal and oral cancers. HPV-associated oral cancers tend to occur in non-smokers and non-drinkers and generally have a better prognosis. Given that HPV infections in the mouth are often asymptomatic and only a small fraction progress to cancer, awareness and monitoring remain essential.
Other factors influencing the transformation of oral potentially malignant disorders (OPMDs) into oral squamous cell carcinoma include mechanical trauma, immune system status, genetic and epigenetic alterations, and microbiota interactions involving viruses, bacteria, and fungi.
Prevention strategies emphasize cessation of tobacco and alcohol use, reduction of betel nut chewing, and vaccination against HPV where applicable. Regular dental examinations, which include thorough inspection of the entire oral cavity, are critical for early identification of suspicious lesions. Dentists and healthcare providers may perform physical examinations and refer patients to specialists such as oral and maxillofacial or ENT surgeons for further evaluation if necessary.
Participation in targeted public health initiatives like Mouth Cancer Action Month raises awareness and encourages timely presentation to healthcare services, ultimately aiming to reduce the burden of oral cancer through prevention and early intervention.
Impact of Early Detection on Treatment Outcomes and Prognosis
Early detection of oral cancer significantly influences treatment outcomes and patient prognosis. Screening tests, while not diagnostic, play a crucial role in identifying patients with abnormal oral findings who require further specialist evaluation, such as tissue biopsy and histopathological diagnosis. An organized screening program with high attendance rates, well-calibrated screeners, quality control, and established referral pathways enhances timely diagnosis and intervention, which is pivotal for improving patient survival.
Raising awareness among patients regarding the signs and symptoms of oral cancer and the importance of regular dental check-ups is essential for early detection. Educational initiatives aimed at medical and dental professionals, including self-instructional courses, have demonstrated some effectiveness in enhancing awareness of early oral cancer detection, although broader implementation and evaluation of these programs remain limited.
Early diagnosis enables prompt biopsy and treatment of persistent oral lesions, which may present with diverse signs and symptoms that can complicate differential diagnosis. Since premalignant lesions, such as leukoplakia, can vary widely in presentation and carry a risk of malignant transformation, careful monitoring and management—including removal of irritants and possible excision of lesions in high-risk areas—are vital to prevent progression to invasive cancer.
Epidemiological data indicate that despite increasing absolute numbers of oral cancer deaths globally, age-standardized mortality rates have remained relatively stable, suggesting that early detection and improved management strategies contribute to controlling mortality rates. However, survival outcomes can vary; for example, younger patients have been reported to experience diminished survival rates, underscoring the complexity of prognostic factors in oral cancer.
Global Incidence, Mortality, and Epidemiological Trends
Mouth and oral cancer rank as the 16th most common cancers worldwide, with notable variations between sexes where it is the 12th most common cancer in men and the 18th in women. Globally, oral cancer caused approximately 199,400 deaths in 2019, more than double the 96,630 deaths reported in 1990. Despite this increase in absolute mortality, the global age-standardized mortality rate (ASMR) has remained relatively stable between 1990 and 2019, reflecting changes in population demographics and healthcare interventions.
Incidence and mortality data are typically reported using age-standardized rates (ASR) to account for differences in age structures across populations. This standardization is crucial since age significantly influences cancer risk. Countries with smaller populations may have higher ASRs but fewer absolute cases, whereas larger populations may exhibit lower ASRs but a greater number of total cases. For example, an ASR of 10 per 100,000 in a population of 100,000 translates to 10 cases, while an ASR of 1 per 100,000 in a population of 10 million equates to 100 cases.
Regional and national variations in incidence and mortality are observed, with certain countries demonstrating higher ASRs for oral cancer, particularly among men. These epidemiological trends are further influenced by risk factors such as tobacco use, alcohol consumption, and infection with high-risk human papillomavirus (HPV) types, notably HPV-16 and HPV-18. Although HPV infection is more strongly linked with oropharyngeal cancers, it also contributes to oral squamous cell carcinoma (OSCC) development, particularly in individuals without traditional risk factors like smoking or drinking.
Understanding these global patterns is essential for targeting screening and prevention efforts effectively. Populations with the highest incidence rates represent the most cost-effective groups for screening programs, facilitating early detection and improved outcomes. Furthermore, molecular studies indicate frequent inactivation of tumor suppressor genes in oral cancer cells, either through mutation or HPV-mediated mechanisms, underscoring the complex biology underlying these cancers.
Challenges and Future Directions
One of the primary challenges in combating oral cancer is the low level of public awareness regarding its early warning signs and the importance of regular screening. Delays in symptomatic patients seeking medical advice contribute significantly to poor survival rates, underscoring the necessity for ongoing public awareness campaigns that encourage early presentation to healthcare services. While campaigns such as Mouth Cancer Action Month have made strides in raising awareness, there remains a need for more widespread and consistent efforts to engage both the public and primary healthcare professionals globally.
Screening for oral cancer faces several obstacles. The effectiveness of screening programs depends heavily on the quality of the screening process, including high attendance rates, proper calibration of screeners, and a robust referral system for patients with suspicious findings. Moreover, screening tests are not diagnostic but serve as a triage to identify individuals requiring further examination and biopsy by specialists. This limitation demands efficient pathways for confirmatory diagnostics and treatment following positive screening results. Additionally, not all screening studies have been rigorously validated against gold standards, which poses challenges in evaluating true screening effectiveness and optimizing protocols.
At the molecular level, advances in genomic analysis have opened promising avenues for improving diagnosis and prognosis. High-resolution genomic profiling can accurately classify the progression risk in low-grade oral premalignant lesions, surpassing conventional histopathological methods that often lack predictive precision. Understanding the molecular mechanisms underlying oral premalignancy and cancer is critical for discovering new diagnostic, prognostic, and predictive markers, as well as for developing targeted therapeutics that could improve patient outcomes. However, translating these molecular insights into clinical practice remains an ongoing challenge.
Future directions emphasize the integration of molecular diagnostics with traditional clinical screening to enhance early detection. The use of adjunctive tools like toluidine blue staining offers a low-cost, noninvasive method to highlight dysplastic or malignant cells during examinations, potentially improving detection rates when combined with clinical judgment. Expanding and refining such adjunctive techniques could contribute to more effective early screening strategies.
Moreover, national and international efforts must continue to develop and implement comprehensive, organized screening programs tailored to diverse populations, especially in high-risk regions. Training healthcare workers, promoting oral self-examination, and leveraging community health networks have shown promise in countries like India and could serve as models for other regions.
The content is provided by Avery Redwood, Lifelong Health Tips